
Republican Senator Lamar Alexander says, "we need to replace Obamacare with insurance choices that allow Tennesseans to select low-cost insurance that fits their budget and their health care needs."
For seventeen years, while residing in Florida, my husband and I had individual health insurance. We moved to the State of Tennessee in 2000. In 2003 our individual health insurance was no longer available in Tennessee. We were unable to purchase individual health insurance through any other company in Tennessee. We called the Tennessee Department of Commerce and Insurance to no avail. They basically told us we would not be able to obtain an individual health insurance policy in Tennessee. Luckily for us, we have a small business with two or more employees and were able to obtain health insurance through the business.
How many people in the State of Tennessee were unable to purchase individual health insurance until the passing of the Affordable Care Act? How many people were unable to get the healthcare they needed since they did not have health insurance? Do you have any idea of the pent up demand in Tennessee since individual health insurance policies were unavailable until recently? Do you really care? I don't think so.
It's no wonder health insurance companies are not making as much money as they were before ACA. There were many people, and still are, in Tennessee who could not even get insurance. Thus, when ACA came along a lot of people were finally able to get health insurance and the healthcare they have been needing for years. If the governments of the State of TN and United States had cared a lot earlier, the demand for healthcare needs may not have cost so much.
I cannot imagine what your idea of a low-cost insurance policy is that fits a budget and health care needs. You who have an excellent health insurance policy paid for by the citizens of the United States.
Thanks, Sen. Alexander for not caring about the health and welfare of the people in your state.
|
Topics:
|
|
Discussing:
- Trump Speech Uses Merit, but Misses Point (1 reply)
- Millionaire tax that inspired Mamdani fuels $5.7 billion haul in Massachusetts (1 reply)
- Trump pardons former Tennessee House speaker convicted of federal public corruption charges (1 reply)
- GOP dereliction of duty, SNAP must be funded (10 replies)
- Electricity prices are rising (3 replies)
- MAP: See the number of SNAP participants by Tennessee county as benefit lapse looms (2 replies)
- Tennessee sheriff defends jailing liberal activist for posting Trump meme (2 replies)
- Terrible things are happening outside. (5 replies)
- Medicare Advantage: Last Week Tonight with John Oliver (1 reply)
- Does Silly Congress care about chaos in cattle market? (4 replies)
- East TN Health Depts. free flu shots today, Oct. 21, 2025 (1 reply)
- Building housing Knox County Democratic Party headquarters up for sale (3 replies)
TN Progressive
- WATCH THIS SPACE. (Left Wing Cracker)
- Report on Blount County, TN, No Kings event (BlountViews)
- America As It Is Right Now (RoaneViews)
- A friend sent this: From Captain McElwee's Tall Tales of Roane County (RoaneViews)
- The Meidas Touch (RoaneViews)
- Massive Security Breach Analysis (RoaneViews)
- (Whitescreek Journal)
- Lee's Fried Chicken in Alcoa closed (BlountViews)
- Alcoa, Hall Rd. Corridor Study meeting, July 30, 2024 (BlountViews)
- My choices in the August election (Left Wing Cracker)
- July 4, 2024 - aka The Twilight Zone (Joe Powell)
- Chef steals food to serve at restaurant? (BlountViews)
TN Politics
- US Senate advances bill to end record-breaking government shutdown (TN Lookout)
- States told by Trump administration to ‘undo’ full SNAP benefits paid for November (TN Lookout)
- New Trump administration rule would override state medical debt protections (TN Lookout)
- US Supreme Court temporarily blocks November SNAP payments (TN Lookout)
- Struggle in US Senate over government shutdown likely to drag through the weekend (TN Lookout)
- Trump administration issues November SNAP benefits, then asks Supreme Court to intervene (TN Lookout)
Knox TN Today
- Basketball fun time: Barnes’ unusual friends (Knox TN Today)
- Lee Ann Hayes: KFD’s sky-diving 2025 Civilian Employee of the Year (Knox TN Today)
- HEADLINES: World news to local Veterans Day Parade & dining (Knox TN Today)
- Meet Rotarian Jyoti Maurya-Brummerstedt (Knox TN Today)
- We are tired of hearing about vaccinations, but … (Knox TN Today)
- Many local teams moved to next round of playoffs (Knox TN Today)
- Clinton High School: Top Fundraising High School (Knox TN Today)
- Insurance or out of pocket for Durable Medical Equipment (Knox TN Today)
- TOA Fountain City Open House is Tuesday (Knox TN Today)
- Pellissippi’s CSI Club hosts Veteran’s Day Breakfast (Knox TN Today)
- Holly Warlick reaches the summit (Knox TN Today)
- Orchid awards + Arbor Day + TVA’s haunted dam ++ (Knox TN Today)
Local TV News
- Warming shelters open in Roane, Greene Counties ahead of cold temperatures (WATE)
- UT adds 368th name to Veterans Memorial during annual wreath-laying (WATE)
- One Knoxville SC to host USL League One Final (WATE)
- Beardsley Farm triples food distribution as SNAP delays increase need in Knoxville (WATE)
- Driver dead after SUV crashes into tree in Claiborne County (WATE)
- Man convicted of 2022 double homicide found guilty of smuggling drugs into jail (WATE)
News Sentinel
State News
- Novonix faces another setback as Stellantis cancels contract - Chattanooga Times Free Press (Times Free Press)
- Chattanooga area full of deals, events honoring military for Veterans Day - Chattanooga Times Free Press (Times Free Press)
- Lookout Mountain display once called ‘Confederama’ closes after 68 years - Chattanooga Times Free Press (Times Free Press)
- Central High will forfeit first-round prep football playoff game - Chattanooga Times Free Press (Times Free Press)
Wire Reports
- Trump administration orders states to pause paying full SNAP benefits - The Washington Post (US News)
- Government shutdown latest: Senate advances a new bill to end the shutdown. Here's what's in it. - Yahoo Finance (US News)
- Trump says he'll issue $2,000 tariff dividend to all except 'high-income people' - abcnews.go.com (US News)
- Asian Traders Cautious on Tech, Shutdown Concerns: Markets Wrap - Bloomberg.com (Business)
- Top BBC bosses resign after criticism of the broadcaster’s editing of a Trump speech - AP News (US News)
- US airlines’ daily cancellations exceed 2,700 as shutdown impact extends - AP News (Business)
- China exempts Nexperia chips from export controls - BBC (Business)
- ByHeart baby formula recalled amid 10-state outbreak of infant botulism - NBC News (Business)
- Some UPS and FedEx planes are grounded. What does that mean for holiday shipping? - NPR (US News)
- Flight Delays: More Than Half Of Flights Disrupted From EWR, LGA, DTW - Forbes (US News)
- 'Ferocious' Winter Storm Could Drop 8 Inches Of Snow Overnight Sunday, Weather Service Says - Block Club Chicago (US News)
- What is Trump’s proposal to pay Americans directly for health care costs? - CNN (US News)
- TechCrunch Mobility: Elon Musk’s threats worked - TechCrunch (Business)
- After selling his business for $532 million, this millennial says a life of leisure was surprisingly ‘boring’, so he’s choosing to back to work - Fortune (Business)
- Many would-be buyers are frozen out of the housing market - NPR (Business)
Local Media
Lost Medicaid Funding
Search and Archives
TN Progressive
Nearby:
- Blount Dems
- Herston TN Family Law
- Inside of Knoxville
- Instapundit
- Jack Lail
- Jim Stovall
- Knox Dems
- MoxCarm Blue Streak
- Outdoor Knoxville
- Pittman Properties
- Reality Me
- Stop Alcoa Parkway
Beyond:
- Nashville Scene
- Nashville Post
- Smart City Memphis
- TN Dems
- TN Journal
- TN Lookout
- Bob Stepno
- Facing South
Single payer
We need a single payer system that delivers real healthcare to the citizens of our nation. The current state policy is nothing more than an instigation of class war between the middle, working and lower classes as to who should get what.
Meanwhile those skimming the profit while contributing virtually nothing to the overall system are laughing all the way to the bank. Until we unite, corporate America will continue to bleed us to death.
I'm still having trouble
I'm still having trouble understanding how insurance companies aren't making money.
US per capita spending for health care is about $9500.
The ACA max deductible is $6850. Estimates for average monthly premiums range from about $400 to $500 before ACA subsidies. Let's call it $400.
So, an individual pays up to $11,650 in premiums and deductibles per year for health care v. the per capita cost of only $9500.
Where is the extra money going?
Football stadiums,
(in reply to R. Neal)
& Baseball stadiums.
Lots of sick people signed
(in reply to R. Neal)
Lots of sick people signed up, causing insurers to bleed money. That's where the money's going.
About 60% of the people who were required to sign up, didn't. Mostly healthy ones, one assumes, leaving an expensive clientele.
Insurers have to hike rates dramatically to cover the cost of claims, which makes more healthy people drop out. It's called an "insurance death spiral."
BCBS is pulling out of most of Tennessee next year. link
Let's clarify that,
(in reply to traveler)
Let's clarify that,
BlueCross BlueShield of Tennessee will not sell individual insurance plans on or off the Affordable Care Act exchange in the state's three largest metro areas next year.
Yes. BCBSTN is not getting
(in reply to bizgrrl)
Yes. BCBSTN is not getting out of the insurance business, just the Obamacare portion they can readily shed.
I'd assumed the thread's context made it clear we were talking about that, but it's better not to assume. Thank you for clarifying.
BCBSTN is not getting out of
(in reply to traveler)
I suggest you try to sign up for a 2017 individual plan out of one of the affected ZIPs before you assert as such.
I don't understand your
(in reply to Andy Axel)
I don't understand your point. As I understand the announcement, BCBS won't be offering individual plans in most metro areas because the new law has made offering such plans untenable.
The move makes sense. BCBS can pull out of the individual market without affecting their main business, employer-based insurance.
Which is different
(in reply to traveler)
from what you said the first time.
BCBS won't be offering
(in reply to traveler)
BCBS won't be offering individual plans in most metro areas because the new law has made offering such plans untenable.
BCBS did not offer individual policies in Tennessee before ACA, at least not in recent times.
The law made offering such plans more feasible. Subsequent piece by piece weakening of the overall program and insurer business practices are why it isn't working.
The insurers are losing
(in reply to R. Neal)
The insurers are losing boatloads of money. That's not 'business practices,' that's simply the result of participating in this government-designed program, complying with its requirements.
Single payer
(in reply to traveler)
Single payer fixes this problem.
Adding third-parties and
(in reply to fischbobber)
Adding third-parties and third-party payers for EVERY medical transaction is at the root of the cost problem.
That problem--cost--is not solved by changing the middlemen from insurance company employee hats to government employee hats. The government employee's hats cost a lot more in every way: money, time, aggravation, quality.
Yes, we've discussed this
(in reply to traveler)
Yes, we've discussed this before. Contributing factors include isolating this pool instead of combining it with small business groups statewide, failure of the risk adjustment, reinsurance and risk corridor provisions intended to mitigate adverse selection, and the state's failure to accept billions in expanded Medicaid funding.
Yes, yes, and yes,
(in reply to R. Neal)
Yes, yes, and yes, except--how does Medicaid expansion relate to the failing exchanges? People permitted on the exchanges make too much money to qualify for the Medicaid expansion anyhow, right?
Drives up provider costs for
(in reply to traveler)
Drives up provider costs for uncompensated care, which drives up overall costs, which drives up premium costs.
Shifting those costs onto the
(in reply to R. Neal)
Shifting those costs onto the taxpayer does the same, just less efficiently and less transparently.
The ultimate problem is cost, which is not fixed by forcing people to buy over-priced insurance so that they can over-pay for over-priced health care.
Adding middle-men, private or public, only increases the cost and eliminates the ordinary price-pressures on sellers of over-priced services.
Wrong
(in reply to traveler)
Single payer fixes the problem. Sanders plan of compulsory participation with a 2/8 employee employer contribution reduces costs and increases coverage for the vast majority of Americans while providing universal care for all. The private sector cannot compete.
Interestingly
(in reply to R. Neal)
The variables you mention would have all been dealt with (at least to a degree) had the state of Tennessee not opted out in favor of Haslam's superior state plan. (What was that plan again?)
Some of the states participating in the ACA are actually seeing rates go down. Of course, most of those states have governments that their citizens actually demand to function.
Also, forget about retiring
Also, forget about retiring early. Pretty soon you won't be able to buy an individual policy (again) and will have to be employed by a company that offers insurance to get any.
Alexander is no stranger to
Alexander is no stranger to peddling DJT Jr's dead elephant party talking points. Consider his erroneous reasons for his hatred of wind power.
I hope you forwarded him your letter.
Worth noting that the ACA has
Worth noting that the ACA has lowered the uninsured rate to an all time low and has cost the fed govt less than expected. (link...)
With no help from Alexander
(in reply to Factchecker)
With no help from Alexander and most other Republicans.
The per-capita cost is much
(in reply to Factchecker)
The per-capita cost is much higher than projected. Roughly double, if I recall correctly. (It has been a while since I did the calculation.)
The program only costs less overall because it has fallen so far short of its enrollment goals.
But it's not surprising that you can entice a bunch of people onto public assistance. The question is whether or not that is a good thing, a 'success.' Once upon a time 'success' meant getting people off assistance, not on it.
Wrong
(in reply to traveler)
Per capita costs had the lowest increase in over twenty years. Even with its flaws, the ACA works better than the previous system.
Those claims are being made,
(in reply to fischbobber)
Those claims are being made, but are bogus or worse.
Critical-thinking check: "How," one asks, "does anyone imagine the ACA lowered costs?" By adding taxes, fees, paperwork, bureaucrats, regs, requirements, and people who don't pay? That's silly.
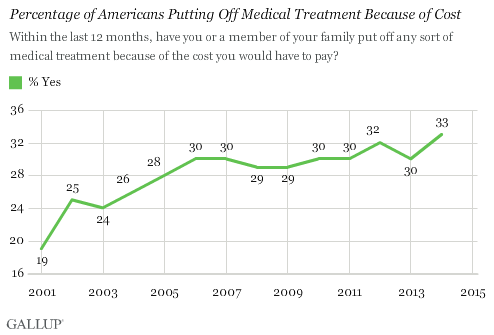
In reality, record numbers of people are putting off needed care due to the higher cost (Gallup).
The excess health care inflation rate(*) is higher, not lower. So when people point to a lower health care inflation rate and credit the ACA, they're pointing to a lower overall inflation rate, not any improvement from the ACA.
*(the growth rate of health care costs; inflation specifically attributable to health care, above and beyond ordinary inflation)
Example: CNBC reports "Overall health spending rose by 5.3 percent in 2014," but the CPI only increased 0.8 percent. BLS That means health care increased a historically-high 4.5 percent faster than inflation.
Also, do not make the mistake of confusing health care spending with the cost of health care--those are not the same. People are buying less because of the higher prices. That is not the same as moderating price increases.
Obamacare has drastically reduced the quality of coverage, too. Despite sharply higher premiums, you now have higher copays and deductibles. That means you're paying more and getting less. Individual policies under Obamacare are beginning to universally resemble the "bad apple" policies the President said we needed Obamacare to replace.
The White House doesn't help. They've been funneling huge payments to the insurance companies under the table to keep down rates on the exchanges. And then, they publicly tout that the artificially-low rates aren't going up as much as expected.
The White House also takes undeserved credit for large numbers of people such as 26-year-old "children" insured on their parents' policy, and others.
It's a mess. But no, it's not better, and it's not holding down increases. Those are flatly false.
So let me get this straight here.
(in reply to traveler)
You make a statement completely absent of any relevant facts, post a chart that shows the implementation of the ACA actually reducing the number of people putting off needed treatment (and the Obama administration dropping the rise of that figure from 11% to 4% while in a recession recovery) and make up a bunch of unsupported conclusions that have no basis in fact?
Anyone can retroactively cherry-pick numbers and arrange them to convince a fool that the black guy is the problem. The bottom line is this. Medical costs were skyrocketing and over 25% of our population was being totally shut out of our system. It wasn't working. It was broken. Obama instituted the Heritage foundation's plan. The one the conservatives wanted to counter Clinton's plan. It doesn't work. But it did stop the bleeding and buy us some time. It's time to elect Clinton and institute a single payer plan for healthcare in this nation.
As to quality of coverage, mine is significantly better. If I use your logic and transpose one anecdotal example as the way the entire system has worked, then it's all better. If I pose examples from the real world, then there are winners and losers. Sorry you're a loser and your participation trophy wasn't enough for you.
How on earth do you conclude
(in reply to fischbobber)
How on earth do you conclude from this
that Obamacare has reduced(!!!) the number of people delaying needed care?
You'd think a successful recovery, low gas prices, and more people insured, with more money in their pockets, should see fewer people delaying needed care. That's sure what we were promised. But that didn't happen.
And it's not gonna to happen.
Obamacare's a shell game. Takes from some, gives it to others. Which does not create more care, or lower the cost.
Adding con men and middle men--government or private--won't fix it. Can't.
People should have been percentage.
(in reply to traveler)
It was an editing error.
Let's not forget though that republicans defeated Hillary's universal plan by promising the private sector would out-perform the public sector. Not only did that not happen, your graph clearly shows the need for a single payer, government run system for our healthcare delivery system. The private sector has not been up to the task.
The program only costs less
(in reply to traveler)
The program only costs less overall because it has fallen so far short of its enrollment goals.
But it has exceeded its goal, if the goal was to increase the percentage of people who have health insurance, which it was. You didn't read the article.
But it's not surprising that you can entice a bunch of people onto public assistance. The question is whether or not that is a good thing, a 'success.' Once upon a time 'success' meant getting people off assistance, not on it.
It's not public assistance. It's a requirement to buy insurance from the private sector. People are griping about the costs, not clamoring for your proverbial "free stuff."
We could have a real debate in this country and in Congress about how to fix the undesirable side effects, starting with costs, but Congress--just like you--doesn't want to do that at all. It would be capitulation for modern Republicans.
"You didn't read the
(in reply to Factchecker)
I did. It's just wrong (or dishonest, you pick which). Sarah Kliff gets consistently low marks for exactly this sort of specious and incomplete 'reporting.' It takes pages and pages of boring explanations correct her.
No, it hasn't exceeded its goal. The "goal" was 24 million on the exchanges by 2016; only 12 million signed up.
And it was supposed to save us $2,500 a year. (Cue the laugh track here...)
If the goal was to "raise everyone's costs a lot to insure not very many people," yes, it has done that in spades.
EXTREMELY BORING PER CAPITA COST CALCULATION
(The media should do this for us, but they don't.)
2013: CBO projected 24 million people would be covered by the now-failing exchanges, (first table, line #9) costing the federal government $96 billion dollars in 2016 (second table, line #2), plus $54 extra billion for 11 million new Medicaid-ers (same tables).
But only 12 million signed up on the exchanges, half of the 24 million CBO projected.
2016: CBO reports $43 billion in subsidies for 12 million exchange people, plus $64 billion for 11 million added to Medicaid. $43 billion + $64 billion = $107 billion total, for 23 million assistance recipients.
SUMMARY
2013 projection: $96 billion + $54 billion = $150 billion projected cost for subsidizing 35 million people. $150 billion / 35 million = $4,300 each.
2016: $107 billion / 23 million people = $4,650 each.
This is what I meant when I said the per-capita costs were higher than promised, and that the overall cost was only lower than projected because the program was failing (people aren't signing up).
(That figure will rise dramatically when the exchanges' new price-hikes get factored into next year's federal subsidy outlays--you heard it here, first.)
Of course it's public assistance. The taxpayers are paying for about 80% of ten million people's health care premiums on the exchanges, and essentially 100% for eleven million added to Medicaid (another federal poverty program). What else can one call that but public assistance? Obamacare is just food stamps for health care.
That's what I'm trying to do. That's why I just spent several hours this morning (which I'll rue this evening, as I work longer on a TGIF to pay back the time) posting links and fact-checking real figures--to try to reach some better understanding between us. All of us. Based on truth, and how to make this really better.
Or we could just cram through whatever broken boondoggle we want with a pack of lies, then gripe about people not liking it and helping us 'fix' it afterwards. It's their fault, you see.
The "undesirable side effects" are inherent. Forcing people to buy insurance to overpay for over-priced medical care does not fix the problem of over-priced medical care. It makes it worse.
Obamacare raises the intrinsic cost of providing care by injecting more steps, costs, overhead, oversight, meddlers, and people who need to be paid into each transaction.
Sorry, I'm not responsible. The people who passed this are. I drove to Washington to oppose it, warning of all the things that are happening, things that you now want me to fix.
It isn't possible. Obamacare was passed on loads and loads of falsities and false promises, of adding benefits while simultaneously reducing middlemen and costs. It does the opposite. That's not my fault.
Snapshot of Where Hillary Clinton and Donald Trump Stand on Seve
from Kaiser Family Foundation ...
Snapshot of Where Hillary Clinton and Donald Trump Stand on Seven Health Care Issues
Sen. Corker jumps in, "This
Sen. Corker jumps in, "This is unwelcome news for more than 131,000 hardworking Tennesseans that will no longer be able to keep their health care plan,” said Corker. “The number of individuals in our state negatively impacted by this law only continues to grow, and with high premiums, rising out-of-pocket costs, and reduced choice, it is clear that the Affordable Care Act is failing Tennesseans.”
How can the ACA be failing Tennessee? Those 131,000 hardworking Tennesseans were more than likely unable to get health insurance before the Affordable Care Act. As of right now, these people can change to Humana. I'm thinking Corker wishes they couldn't get insurance at all and were glad when they couldn't get insurance before ACA. He's just being cruel in the name of politics.
I personally believe the
(in reply to bizgrrl)
I personally believe the Affordable Care Act is failing the entire country by making health care less affordable and less efficiently delivered.
Removing people's choices removes their ability to preferentially patronize the better, more cost-efficient providers, which in turn removes the providers' incentive to innovate or reduce costs.
The central problem is cost, which Obamacare makes worse.
A lady told me today that her doctor had pecked away at a tablet computer through her entire (recent) appointment, rather than paying attention to her. When asked what he was doing, the doctor replied, bitterly, that he was filling out her Obamacare-mandated electronic health record.
That adds cost.
OMG, he's back. Pretty sure
(in reply to traveler)
OMG, he's back.
Pretty sure that is the doctor's choice. My doctor doesn't do that.
Obamacare put about 13,000,000 more people on health insurance.
Don't pay attention to him.
(in reply to bizgrrl)
He doesn't understand the industry. I didn't even attempt to explain the fundamentals of actuarial tables and how costs and rates are derived.
Traveler is a simpleton attempting to understand a complex problem at a grade school level. He will hold his breath and cry neener neener when you lay down facts.
I'd think that only a
(in reply to fischbobber)
I'd think that only a simpleton over-awed by his topic would imagine that how insurers derive their rates matters to the question of whether an imposed policy (Obamacare) affects the insurers' costs. The costs and rates are a consequence of the policy, but you'd muddle those consequences in as a pseudo-causation.
But speaking of, the Society of Actuaries projected Obamacare would raise the insurers' cost of individual claims 32%.
And it happened. For all the reasons they said. And more. So you're just flat wrong if you think Obamacare reduced cost. Both theory and practice show otherwise.
As for trying to understand a complex problem at a grade-school level, I find the proponents' thinking faith-based and uncritical. "If we force everyone to buy over-priced health care--and hire loads of middle-men and bureaucrats to do it, hurray!--that'll chop health care costs!" It didn't work? "We need more middlemen! And subsidies!"
That's beneath grade-school level, but feel free to defend it. Feel free to explain how Obamacare's alchemists and Grubers magically lower premiums, deductibles, and co-pays by adding services, middlemen, taxes, fees, reporting, obstacles, and requirements to health care.
Be sure to cc: those big-league professional insurers pulling out of the Obamacare exchanges so they'll understand that they actually made a killing losing 50%, etc.
The doctor in question said
(in reply to bizgrrl)
The doctor in question said it was a requirement of Obamacare's electronic health records, which squares with the law. Google HIT and EHR.
I know it's an article of faith that getting people on the dole is a great good, a service to humanity, but I think people are happier and better-served getting off welfare rather than trapped in it.
Obamacare has swelled Medicaid by 11 million (including some who were previously insured), and is now subsidizing care for 10 million people on the exchanges. It is a giant welfare-program, a handout--public assistance--plain and simple.
The doctor in question said
(in reply to traveler)
The doctor in question said it was a requirement of Obamacare's electronic health records, which squares with the law
Yes, electronic health records are required. It doesn't mean the doctor has to spend patient time on the computer. My physician'office is meeting the electronic records requirements without my doctor staring at a computer during my patient visit.
Electronic record keeping
(in reply to traveler)
The private sector is failing miserably at adapting to electronic record keeping and incorporating into the private sector insurance system.
My doctor left the private sector to go work at Y-12 in a socialized medicine capacity because the government medical systems are simply more efficient and allow doctors to do their job, instead of spending all their time on billing.
The government hasn't gotten
(in reply to fischbobber)
The government hasn't gotten its Obamacare website working even to this day. You're arguing they're more sophisticated, competent, more efficient technologists?
Numerous studies have shown that EHRs waste time, reduce the number of patients doctors can see each day, add to overall costs. Most doctors hate 'em, and yours is plainly happier not having to keep them. But underlings do, and the cost is still there, hidden, only greater.
But this all goes to the sheer arrogance of Obamacare, presuming to tell doctors how to keep their records. As if the bureaucrats knew how to do the doctors' jobs better than the doctors do. Stupid people, taking charge. And think they can do better. It's the fatal conceit. Stunning.
If you can't see the value of
(in reply to traveler)
If you can't see the value of electronic medical records in terms of patient service, safety and outcomes then you must not go to the doctor much.
I have already seen the benefits of better and more efficient coordination, communications and information sharing among my doctors.
As with any change to something new, there are often problems with implementation. The current issues appear related mostly to interoperability and ease of use. These kinks will get worked out as users, regulators, professional associations, standards organizations and system builders/integrators gain more experience.
There are also cost concerns, but I believe there are incentives available to help.
Maybe you haven't had my
(in reply to R. Neal)
Maybe you haven't had my experience (and family's, this past week), which is that your doctor now spends your appointment looking at their EHR tablet, pecking away at all the check-boxes that pop up as the tablet guides him/her through an Obamacare-mandated computer-support-from-India style interview, instead of looking at and listening to their patient.
That does NOT improve patient care. That wastes precious time and leads to missed diagnoses and dreadful mistakes. Typing and typing, then typing more things into a computer isn't what makes the patient better.
Of course I see the potential advantages, I just think it's incredibly arrogant for self-important fatheads to impose their fatheaded edicts on everyone. Doctors aren't stupid. If they see that a new aid helps them deliver better, more efficient care, you don't have to force them, they use it.
We shouldn't presume to tell doctors how to run their practices or what tools to use, any more than have the federal government dictate internal database formats to software developers, or prescribe required hammer technique to blacksmiths. The people who actually do it for a living can figure it out, collectively, far better. American innovation depends on that.
Maybe you haven't had my
(in reply to traveler)
Maybe you haven't had my experience (and family's, this past week), which is that your doctor now spends your appointment looking at their EHR tablet, pecking away at all the check-boxes...
Actually, I have. I changed doctors.
The new doctor (specialist) probably saved my life. He also has a notebook but he talks to me, not it.
The first doctor was like Groundhog Day. Even though he had it all there on his computer, which he stared at and fidgeted with, he didn't remember why I was there, what procedures he'd done, what medications he'd prescribed, etc. It was like starting over on every visit. That's not a problem with ACA and EHR. That's a problem with the doctor.
Turning doctors into clerks
(in reply to traveler)
You give the ACA too much credit. Insurance companies and corporations determine how records are kept, the ACA mandates that they be standardized and accessible.
Virtually all of the inefficiencies you've described have been the direct result of institution that was designed to fail. Insurance companies and medical corporations have determined that by jamming the system they can achieve a self fulfilling prophecy of inefficiency. We saw the same wailing and gnashing of teeth in the transportation industry when we first automated our records. In less than five years, we could track a package in real time from destination to delivery in real time. That's not immediate. That took five years. But it works pretty good now, industry wide. The medical profession is behind. They need to automate their records.
Coming up with isolated anecdotes or commenting on the obvious, (Where are overworked office staffers supposed to find the time?) doesn't change that reality.
Looks open to me.
(in reply to traveler)
(link...)
That's the user data-entry
(in reply to fischbobber)
That's the user data-entry interface, basically a web-based application form. Trivial. (Which, amazingly, the feds couldn't even get that working for 2013's roll-out despite having spent hundreds of millions of dollars and *years* to do it.)
The remaining 80% of the website that actually processes that user data--despite billions spent--is still not done.
Initially they were doing the behind-the-scenes processing all by hand, manually printing out each application. (This was all legally supposed and repeatedly promised to be working by Oct. 1, 2013.)
Complete idiots. An absolute monument to government--utter incompetence.
Not really. Projects of this
(in reply to traveler)
Not really. Projects of this magnitude always take longer than expected whether in the public or private sector. In addition, these types of projects are constantly fine-tuned. This type of change has affected almost every industry. It is time for the health care industry to move into the 21st century.
Removing people's choices
(in reply to traveler)
This statement ignores the fact that many of the pre-ACA 'plans' were actually devices by which insurance companies charged customers an incredibly reasonable rate because those plans covered very little and paid out very little, leaving customers effectively uninsured (for a reasonable fee). That does nothing to control costs.
It probably does, in the short term. Of course, you're conveniently ignoring the benefit in that particular cost-benefit calculation. Pre-ACA, record-keeping in medical practice was stubbornly anchored in the 19th century. Your medical records were illegibly hand-written and kept in a paper file, which was marginally useful, so long as you only ever went to that one doctor's office. Have more than one doctor? Switch primary care doctors over time? Those records become exponentially more useless, as information is either not transferred or becomes garbled because nobody can read that notoriously bad physician handwriting. Think about it. Each time a patient goes to a different doctor's office, he or she is asked to fill out, from memory, a questionnaire, detailing current and past conditions, treatments, surgeries, allergies, medications, and whatnot. Forgot to mention you once had an allergic reaction to penicillin? 'That was eight years ago. I didn't think it was important.' Perhaps that's what they'll write on your headstone.
That iPad represents vastly more accurate and more accessible medical records. You have to be be willfully ignorant to believe that this won't result in more efficient and more effective healthcare, which will save costs. Oh, and it'll save lives, too.
This statement ignores the
(in reply to Somebody)
Raising the deductibles (as Obamacare has done) prods more and more people into shopping for care. But previously people voluntarily chose this and stashed the savings in health savings accounts. Now they pay higher premiums, save nothing, and face higher expenses even with 'comprehensive' Obamacare insurance that costs a bundle.
I know from first-hand experience that's a pile of nonsense. I spent winter and spring of this year, every day for months locked in battle together with people using those records, and caught errors over, and over, and over. Bogus entries, missed data; workers, distracted by their record-keeping duties, missing life-threatening emergencies. I SAW it. Huge time-waste, and they HATED it.
But if you want a more public example, that Ebola patient (Duncan) who went the the Dallas ER? His EHR, laboriously entered, had all the data from his first visit to suggest Ebola, but no one read it. They sent him home with acetaminophen and antibiotics instead.
(link...)
1,400 pages of records--who can read that? Two nurses got Ebola.
Imagining what's good for others is exactly the problem with government mandates--people who don't know, commanding the ones who do.
Medical Industry
(in reply to traveler)
You are describing the medical industry and blaming it on the ACA. Virtually every circumstance you've described is rooted in billing, not patient care. As you are, no doubt, well aware, the ACA has still not been fully instituted. Any judgement as to whether or not it will operate effectively once all the states participate is highly premature.
Plus you've conveniently tried to push every patient into the same circumstance. My coverage increased and my deductibles went down under the ACA. Why? Because many of the people covered under my policy were in states that participated in the ACA and as a result my individual treatment cost went down. Tennessee doesn't participate in the ACA and our rate increases are directly tied to the federal money that we refused. Someone has to pay for this service.
As to your point that HSAs are no longer available to consumers, that is a state, not federal issue. (link...) Our exchange could have easily been designed to incorporate this factor into our exchanges if our governor had gotten off his dead ass and done his job.
"As to your point that HSAs
(in reply to fischbobber)
I agree with your author that limiting premium assistance to silver plans was asinine--why discourage, in law, people from bargain-hunting? But a lot if not most of Obamacare is like that. I can only assume insurers said they needed that guarantee of higher subsidy revenue (insurers' share of the Obamacare subsidies is reduced if people choose minimal policies).
I can't square your statements on HSAs with the law. The ACA itself sets a low legal limit on the highest deductible you can buy--state policy doesn't enter into it.
Previously you could buy a $10,000-deductible plan if you wanted, now you can't. That effectively wipes out the purpose of an HSA, which was to buy cheap insurance against major medical expense and pay cash for your ordinary needs. That's rather pointless when then the law forces you to buy (and pay for) comprehensive insurance anyhow.
The Obama Administration, meanwhile, hostile to choice and competition, has been doing its level Machiavellian best to wipe out HSAs entirely by writing 'rules' (regulations) that make them impossible.
link
How California is making
How California is making Obamacare work...
(link...)
Bleeding - econ opinion v science, poor people as parasites
"Lots of sick people signed up, causing insurers to bleed money. That's where the money's going.
------------------------------------------------
The hideously downtrodden insurance companies are bleeding money because poor people signed up for health insurance.
1) What is the role that profit, err, "surplus"-taking plays in the American health care market by "non-profits" like BCBS- how are premiums, drug costs and other health system components' prices influenced by non-profits and private capital needing to make a profit?
2) How does market failure affect the american health system and what happens when there is not government intervention?
3) Medical loss ratios and health insurance companies - up or down?
4) $300 million on new BCBS headquarters vs rate reductions?
5) Operating reserve ratios?
Below are BCBS of Tennessee yearly bleeding, sorry, surplus numbers, in thousands, from their 2015 financial statements
2014 - 2,434,774
2015 - 2,434,606
Here's Wendell Potter (link...) on the horrifying prospect faced by companies like BCBS and Aetna of having to cope with the new regime.
"Here, for example, is the grim news Aetna’s CEO, Mark Bertolini, delivered to Wall Street financial analysts a few days ago:
'In light of a second-quarter pretax loss of $200 million and total pretax losses of more than $430 million since January 2014 in our individual products, we have decided to reduce our individual public exchange presence in 2017, which will limit our financial exposure.'
This despite the fact that since January 2014, the date Bertolini mentioned above, Aetna has reported operating profits of $6.7 billion. That’s right. Even though Bertolini said Aetna hasn’t yet turned a profit on its Obamacare business, overall it has pocketed nearly $7 billion."
The fact that a company is
(in reply to right wing hax)
The fact that a company is making money in another business or market is rather irrelevant. If they lose loads of money selling a product, or selling in a new, artificial 'market,' they do exactly what you'd do--they quit.
Healthcare is not a traditional market
(in reply to traveler)
The reason we are the only industrialized nation that treat healthcare as a for profit market is because it is not a traditional market. I can eat peanut butter instead of meat to cut back on my food budget, but I can't decide to treaty a sinus infection if I have stage II colon cancer.
This is what makes your entire argument so stupid. You are willfully ignoring the entire purpose of health coverage to begin with and doggedly insist that the point of the system is to run at a profit. It's not. The point of the system is to provide healthcare to the American people and those trying to do it at a profit have screwed it up. If they'd done their job to begin with the government wouldn't be involved.